
"Thank you for giving me options. It gave me trust in myself that I can recover from my addiction." - Participant in The Acceptance Project
In brief
Stigma against people with mental health and substance use problems in healthcare settings is a public health issue. Studies have found that it can result in clients receiving insufficient information, not being included in decision-making, or being patronized and/or humiliated. In particular, evidence has shown that burnt-out or tired service providers can be more stigmatizing towards people with mental health and substance use problems.
CHCs are an optimal setting for projects aimed at reducing stigma as they cater to a diverse population, which often includes Toronto’s most vulnerable and marginalized groups. CHCs offer a wide range of services and programs such as medical, dental, counselling/social work, nutrition, and recreation programs.
This issue of Evidence in Action features The Acceptance Project, a stigma-reduction intervention for community health centre staff. Evidence in Action profiles knowledge generation, exchange, and implementation activities across Ontario.
Read it below or download the PDF.
Background
Stigma has a negative effect on people with mental health and substance use problems worldwide and is a significant barrier to getting appropriate care. Stigma can lead to:
- difficulty accessing resources and services, such as employment and housing;
- social isolation due to exclusion from activities; and
- low levels of health service utilization.
Stigma against people with mental health and substance use problems in healthcare settings is a public health issue.
Studies have found that it can result in clients receiving insufficient information, not being included in decision-making, or being patronized and/or humiliated. In particular, evidence has shown that burnt-out or tired service providers can be more stigmatizing towards people with mental health and substance use problems.
A study funded by the Canadian Institutes for Health Research used a cluster, randomized controlled trial design to test the effectiveness of an anti-stigma intervention targeting staff in six community health centres (CHCs).

CHCs are an optimal setting for projects aimed at reducing stigma as they cater to a diverse population, which often includes Toronto’s most vulnerable and marginalized groups. CHCs offer a wide range of services and programs such as medical, dental, counselling/social work, nutrition, and recreation programs.
A pilot project, for which this current initiative was based, set out to develop an anti-stigma intervention for primary care staff. With the guidance of staff and service users at three CHCs in Toronto, a five-pronged intervention was developed.
As this project was met with some success, the research team decided to scientifically test the intervention using a randomized controlled research design.
For this study, six CHCs were randomly assigned to receive the intervention over the course of three years and three CHCs were in the control group and did not receive the intervention.
The aim was to determine the effects of the intervention on stigmatizing attitudes and behaviours toward clients with mental health and substance use problems.
The CHCs that received the intervention were as follows:
- Stonegate CHC
- TAIBU CHC
- Rexdale CHC
- The CHCs in the control group were:
- Black Creek CHC
- Women’s Health in Women’s Hands
- LAMP CHC
The researchers also did in-depth situational assessments of each CHC to document their services, programs, governance, and demography.

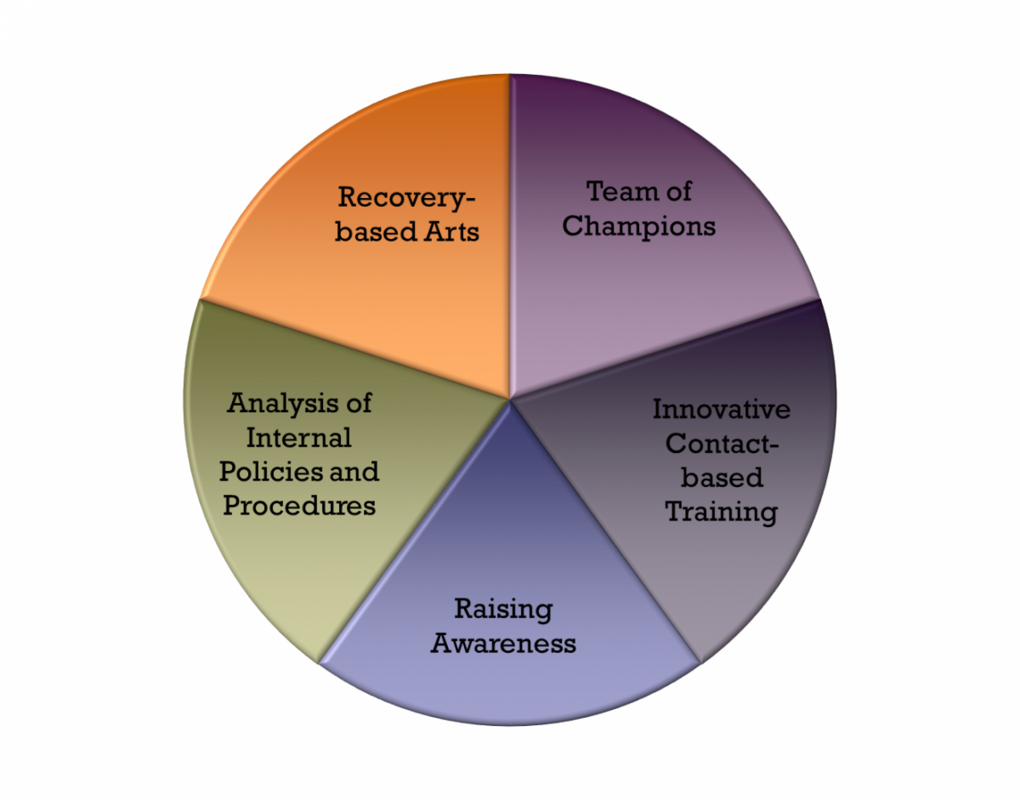
The intervention
The intervention had five components, each emphasizing a contact-based approach. This means that people with lived experience of mental health and/or substance use issues played a vital role in the development, participation, and presentation of the intervention.
Team of champions
Each CHC in the intervention group had three to five staff members who acted as champions of the project. Their role was primarily to support and encourage participation in the project and raise awareness about stigma within their CHC.
Contact-based training
Four training sessions were held for all staff members in the intervention group. The sessions included academic facilitators as well as a person with lived experience. Topics included (but were not limited to):
- concepts of stigma;
- social location (a person’s place in society defined by characteristics such as gender, ethnicity, or religion);
- intersecting stigma (the process of many identities such as sexual orientation or ethnicity being stigmatized at the same time); and
- the importance of staff taking time for self-care and reflection.
Raising awareness
Staff in the intervention CHCs created posters to raise awareness about mental health and stigma among clients and staff. Through discussions with staff, it was determined that the posters would include an image of a CHC client with lived experience as well as a quote indicating how the CHC had helped them. The posters were displayed in various areas of the CHCs.
The champions and project team members also created a logo and corresponding tagline, which were displayed on items such as pens and buttons. The logo consists of two people embracing, to emphasize the idea of acceptance.
Analysis of policies and procedures
The researchers analyzed some of the CHC’s policies and procedures to find out if they reflected anti-stigma practices and protocols. The analysis tool allowed the project team to highlight areas that required attention. CHC senior management then reviewed the analysis and agreed to implement the changes in their policies and guidelines.
Recovery-based arts

The final component of the intervention was the recovery-based arts program. For this element, staff members and clients participated in a 10-week art class taught by a staff facilitator and an artist. Each week the class focused on a theme related to the experience of stigma. The classes consisted of 10 clients with lived experience and three staff members. To create a safe and trusting environment, the same 13 people would participate in the class each week.
At the end of the 10 weeks, an art show was held and all CHC staff members were asked to attend. Participants were encouraged to speak about their work and what it was like to be in the program. The goal was to allow staff and clients to learn about each other on a deeper level and to create art as a way of expressing and understanding stigma.
The research
Staff members from each CHC and clients were asked to complete a questionnaire at four different time points during the three year project period and participated in interviews to measure stigmatizing attitudes and behaviours. In total, 392 staff and 89 clients completed the surveys, and 18 staff and 25 clients participated in interviews.
Two of the scales that staff completed (Opening Minds Scale for Health Care Providers and the Mental Illness: Clinicians Attitudes Scale) found significant differences between the intervention and control CHCs. Staff members who received the intervention had significantly greater reductions in stigma compared to the controls. The control group scores essentially stayed the same throughout the study period, with little change in the way staff treated clients with mental health and/or substance use problems.
Client data were harder to analyze because it was a small group, so it was difficult to draw conclusions from the results. But the results did suggest there were greater reductions in stigma at the intervention sites than at the control sites.
The application
In follow-up meetings, staff members from the intervention sites reported that the initiative had changed and would continue to change their practice. One of the biggest changes they reported was to self-care. After they received the intervention, providers reported that they were having more discussions about mental health and substance use, and more of them said they talked about their own health and about taking steps to improve their wellbeing. Such discussions with colleagues humanize the experience of living with a mental health or substance use problem.
A complete paper and electronic package with all components of the intervention will be provided to all participating CHC sites so they can continue to use these tools to promote an anti-stigmatizing workplace.
Lessons learned
Although the intervention did show statistically significant improvements in the stigmatizing attitudes and behaviours of staff toward clients with mental health and substance use problems, it was not possible to determine which components of the intervention worked best, or if it needs to be implemented in its entirety for successful results. It was also difficult to determine if the intervention worked best at the individual level or at an organizational level.
The primary goal of the project was to reduce stigma within the CHCs rather than in individual staff members. Therefore, more time may be needed to determine if the intervention successfully changes attitudes and behaviours on a larger scale. Regular ‘booster’ sessions are commonly held for intervention such as this, so conducting all or part of the intervention at various time intervals may prove to be a good way to reduce stigma.
For more information about this important project, please contact Emily Lentinello, Special Advisor/Project Coordinator, Emily.Lentinello@camh.ca.
Author: Emily Lentinello